Hospital infrastructure operates on a foundation of invisible complexity. Behind every controlled room temperature, every sterile airlock, every uninterrupted power supply, and every automated pharmacy dispenser lies a sophisticated control system making thousands of decisions per second. Two technologies dominate this landscape: the Distributed Control System (DCS) and the Programmable Logic Controller (PLC). For healthcare facility managers, biomedical engineers, and hospital automation specialists, understanding the distinction between these platforms is not merely academic — it directly determines patient safety, regulatory compliance, and operational resilience. This guide breaks down how DCS and PLC architectures differ, where each excels in hospital environments, and how modern facilities are leveraging both through integrated automation strategies.
Struggling to manage maintenance across your hospital's control infrastructure? Oxmaint CMMS helps healthcare teams track DCS and PLC assets, automate work orders, and stay audit-ready.
What Is a Distributed Control System (DCS)?
A Distributed Control System is an automated control platform designed to manage complex, continuous processes across large physical environments. Unlike centralized systems, a DCS distributes intelligence across multiple controllers — each responsible for a defined zone or subsystem — while a central supervisory layer integrates all data into a unified operational view. In hospital settings, DCS architectures are most commonly found managing building-wide HVAC systems, medical gas networks, chilled water plants, and central energy management platforms.
The defining characteristic of a DCS is its emphasis on process continuity and system-wide coordination. When a hospital's DCS detects a pressure drop in a negative-pressure isolation room, it does not simply trigger a local alarm — it simultaneously adjusts air handling unit setpoints, reconfigures exhaust fan speeds across the affected wing, and logs the event with timestamp data for infection control review. This coordinated, multi-node response is what sets DCS apart from simpler control architectures. The system is purpose-built for environments where subsystems are deeply interdependent and where process stability matters more than microsecond response times.
What Is a Programmable Logic Controller (PLC)?
A Programmable Logic Controller is a rugged industrial computer designed to execute discrete, logic-based control tasks with extreme reliability and speed. PLCs operate on ladder logic or structured text programs that evaluate input conditions and trigger output responses in deterministic, millisecond-level cycles. In hospital infrastructure, PLCs are the workhorses behind individual equipment control: elevator interlocks, sterilizer cycle management, generator automatic transfer switches, fire suppression panel interfaces, and medical equipment bay power sequencing.
PLCs excel at precise, repeatable tasks with clear binary outcomes — open this valve, start this pump, engage this relay. Their strength is not in managing sprawling process networks but in executing a defined sequence of actions with absolute precision and fault tolerance. A PLC controlling a hospital's autoclave sterilization cycle must hit exact temperature and pressure thresholds at precise intervals, log every deviation, and halt the process safely if parameters fall outside specification. This is logic-intensive, safety-critical work where the PLC's deterministic execution model is exactly the right tool.
DCS vs PLC: Core Architecture Comparison
- Manages continuous, process-oriented workflows
- Distributed intelligence across multiple controllers
- Native multi-loop process coordination
- Built-in historian and trend logging
- Designed for large-scale, campus-wide deployment
- Response time: 100ms to 1 second range
- Manages discrete, sequential logic tasks
- Localized control with standalone operation
- High-speed scan cycles for rapid response
- Modular I/O expansion for equipment integration
- Cost-effective for individual equipment control
- Response time: 1ms to 10ms range
Where DCS Fits in Hospital Infrastructure
Modern hospitals are among the most energy-intensive buildings in the world, consuming two to three times more energy per square foot than commercial office buildings. Managing this energy profile while maintaining precise environmental conditions across operating theaters, intensive care units, clean rooms, and laboratory spaces demands the coordinated, adaptive control that only a DCS can deliver.
Hospital HVAC automation is the primary domain of DCS deployment in healthcare. The system continuously modulates air handling units, cooling towers, variable air volume boxes, and humidification systems to maintain temperature tolerances of ±1°F and relative humidity within ±5% across hundreds of zones simultaneously. Operating rooms require 20 air changes per hour with HEPA filtration. Pharmacy clean rooms must sustain ISO Class 5 or better particulate conditions. Isolation rooms need precisely maintained negative or positive pressure differentials. A DCS orchestrates all of these requirements from a single integrated platform while automatically adjusting for occupancy patterns, outdoor conditions, and real-time energy pricing signals.
Beyond HVAC, DCS platforms in hospitals manage central utility plants — the chilled water, hot water, and steam systems that feed building-wide conditioning. Central energy management, power quality monitoring, and integration with hospital information systems for demand response programs all run through the DCS layer. When a hospital's DCS integrates with its Building Management System (BMS), facility teams gain complete visibility into every energy-consuming asset from a unified dashboard, enabling preventive maintenance triggers based on real performance trends rather than fixed schedules.
Hospitals managing multiple DCS assets across campus need a single platform to track calibration schedules, work orders, and compliance records — sign up for Oxmaint and start building your control system maintenance program today.
Where PLCs Dominate in Healthcare Facilities
Step into any hospital mechanical room, central sterile supply department, or rooftop electrical switchgear vault and you will find PLCs at the core of equipment control. The deterministic, high-speed logic execution that PLCs provide is irreplaceable for safety-critical equipment where response latency cannot be tolerated.
Automatic Transfer Switches (ATS) that shift hospital power loads from utility feeds to emergency generators during an outage rely on PLC logic to execute the transfer within 10 seconds — the maximum acceptable window for life safety systems under NFPA 99 and NEC Article 517. Steam sterilizers and autoclaves in central sterile supply use PLCs to manage pressure ramping, temperature hold phases, and vacuum drying cycles with exact parameter control and IQ/OQ/PQ validation documentation. Elevator control panels in healthcare facilities use PLC-based logic to manage fireman's service, emergency power recall, and door timing sequences that must meet ADA and life safety code requirements simultaneously.
Laboratory automation systems — automated specimen sorters, centrifuge stations, and pneumatic tube networks for lab sample transport — are predominantly PLC-controlled. The pneumatic tube systems that carry blood samples, medications, and documents across hospital campuses at speeds up to 25 feet per second require PLC logic managing carrier routing, station interlocking, speed control, and jam detection with sub-10ms response cycles. Any control architecture with slower response characteristics would result in carrier collisions and specimen loss.
Hospital System Control Architecture Map
Key Technical Differences That Matter for Healthcare
The DCS versus PLC debate in hospital environments ultimately comes down to five technical dimensions: scalability, redundancy architecture, response time requirements, programming complexity, and integration capability. Each dimension carries different weight depending on the specific hospital application being evaluated.
Scalability strongly favors DCS for hospital-wide deployments. A DCS can manage thousands of control loops and I/O points across multiple buildings from a unified engineering workstation. Expanding a PLC-based system to comparable scale requires engineering and commissioning each additional PLC independently, which multiplies both cost and complexity. For a new hospital campus adding a medical office building or an ambulatory surgery center, extending the existing DCS to cover the new facility is significantly more efficient than deploying parallel standalone PLC networks.
Redundancy is built into DCS architecture as a native feature. Hospital-grade DCS platforms offer redundant controllers, redundant communications networks, and redundant I/O modules that fail over automatically without process interruption. PLCs can be configured with redundancy, but it requires additional hardware investment and careful engineering. For life-safety systems like hospital HVAC serving operating rooms or ICUs, the inherent redundancy of a DCS provides a stronger reliability foundation.
Response time reverses this advantage for many hospital applications. PLCs execute scan cycles in 1 to 10 milliseconds — fast enough for generator transfer switching and sterilizer pressure control. DCS response times of 100 milliseconds to one second are perfectly adequate for HVAC trim and energy management but would be unacceptable for equipment protection logic requiring microsecond-level response.
DCS vs PLC Hospital Application Matrix
| Hospital Application | Preferred System | Primary Reason | Maintenance Interval |
|---|---|---|---|
| Campus HVAC Automation | DCS | Multi-loop process coordination | Quarterly calibration |
| Generator ATS Control | PLC | Sub-10ms transfer speed | Monthly functional test |
| Central Sterile Supply | PLC | Precise cycle sequencing | Weekly parameter verification |
| Medical Gas Monitoring | DCS | Campus-wide integration | Monthly sensor check |
| OR Environment Control | DCS / Hybrid | Zone coordination + interlocks | Monthly calibration |
| Pneumatic Tube System | PLC | High-speed routing logic | Bi-weekly inspection |
| Energy Management | DCS | Multi-system optimization | Annual software review |
| Fire Suppression Interface | PLC | Deterministic safety logic | Semi-annual test |
Integration: When DCS and PLC Work Together
The most sophisticated hospital automation environments do not choose between DCS and PLC — they integrate both into a layered architecture where each technology operates in its natural domain. A hospital's DCS serves as the supervisory layer, collecting data from PLC-controlled equipment and presenting a unified operational view to facility management. PLCs handle the fast, safety-critical sequences while the DCS manages the broader process coordination and reporting.
In a hospital operating room suite, this integration looks like the following: individual PLCs manage the airlock interlocking sequences between the clean corridor and each OR, ensuring doors cannot simultaneously open and compromise pressure relationships. The DCS simultaneously monitors all OR room pressures, adjusts AHU supply air volumes across the suite based on occupancy schedules, coordinates with the chilled water plant to optimize cooling efficiency, and logs environmental data for Joint Commission compliance documentation. Neither system alone could deliver both the safety logic speed and the process-wide coordination that this application demands.
Modern communication protocols — OPC-UA, BACnet, and Modbus TCP — make DCS-PLC integration straightforward for experienced system integrators. Hospital facility managers should ensure that their automation vendors provide documented integration architectures and maintain cybersecurity standards appropriate for healthcare networks, where control system communications can potentially intersect with clinical IT infrastructure.
Maintenance and CMMS Management for Control Systems
Both DCS and PLC systems require structured preventive maintenance programs to sustain reliability in hospital environments. DCS platforms need periodic backup verification of controller configurations, calibration of field instruments including temperature sensors, pressure transmitters, and flow meters, and software patch management coordinated with facility downtime windows. PLC systems require scan time verification, I/O module functional testing, battery backup replacement for program retention, and logic review when connected equipment is modified or replaced.
Tracking maintenance activities across a hospital's complete control system inventory — which may include hundreds of PLC panels and dozens of DCS controllers distributed across a campus — requires a CMMS platform capable of managing complex asset hierarchies. Work orders for DCS calibration tasks must link to the specific field instruments, the engineering workstation software version, and the commissioning documentation package. PLC maintenance records must capture the program version, I/O count, connected equipment assets, and the technician's observations during testing. Without this structured documentation, facilities face compounding risk during Joint Commission surveys and NFPA 99 inspections.
Want to see exactly how a CMMS handles DCS and PLC asset workflows? Oxmaint gives your team live preventive maintenance scheduling, compliance report generation, and custom asset profiles for control system equipment.
Compliance and Audit Readiness in Healthcare
Hospital control systems operate under a demanding regulatory framework. NFPA 99 Health Care Facilities Code governs the testing and maintenance requirements for essential electrical systems, medical gas systems, and HVAC systems in healthcare facilities. The Joint Commission's Environment of Care standards require documented evidence that life safety systems including emergency power, fire protection, and ventilation perform within specification on a scheduled basis. CMS Conditions of Participation extend these requirements to all facilities participating in Medicare and Medicaid programs.
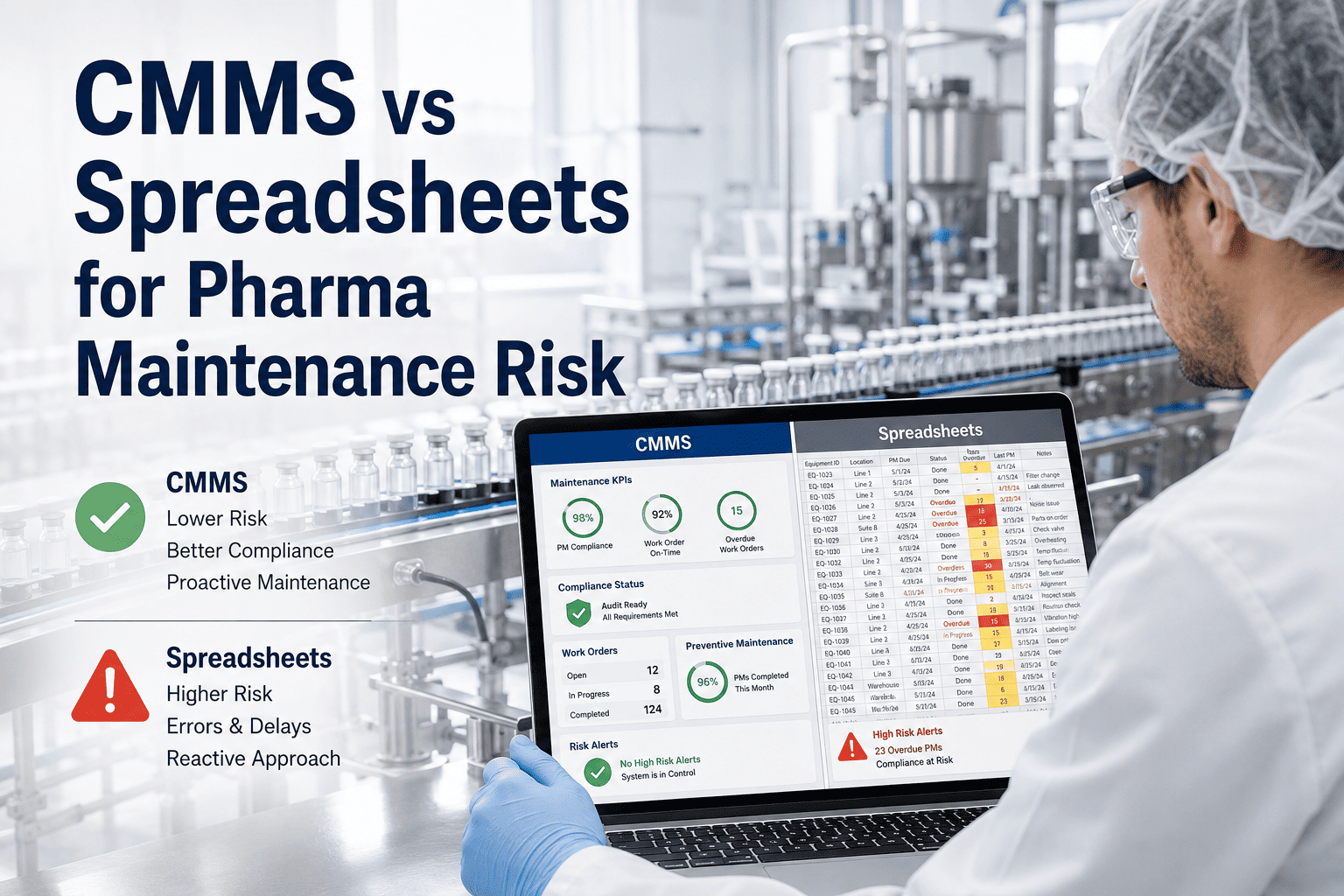
For PLC-controlled systems, surveyors focus heavily on functional test documentation for emergency generators, ATS panels, and fire suppression interfaces. Every test must capture the date, technician identity, test parameters, results, and corrective actions for any failures. DCS-managed systems face scrutiny around calibration records for environmental monitoring instruments, software change management logs, and alarm response documentation. Facilities that rely on paper logs or disconnected spreadsheets for these records routinely struggle during surveys, spending hours reconstructing documentation trails that a properly configured CMMS would surface in seconds.
Choosing the Right Control Strategy for New Hospital Projects
For hospitals undertaking new construction or major renovation projects, the DCS versus PLC decision should be made early in the design development phase, ideally during the 30% construction documents stage when mechanical and electrical systems are being specified. Several factors should drive this decision beyond pure technical capability.
Total cost of ownership over a 20-year asset lifecycle often favors DCS for large, complex facilities despite higher initial capital cost, because ongoing engineering labor for system modifications and expansions is significantly lower. Smaller critical access hospitals or ambulatory surgery centers may find that a well-integrated PLC-based BMS with SCADA visualization delivers sufficient capability at a fraction of the DCS infrastructure cost. The facility's in-house engineering and facilities management capability also matters — DCS platforms require specialized training and can create vendor dependency if internal expertise is not developed alongside implementation.
Hybrid architectures that position a DCS as the supervisory and process control layer while deploying PLCs for equipment-level safety logic represent the approach most commonly specified by healthcare facility design engineers today. This strategy captures the strengths of both platforms while managing complexity and cost within a coherent, maintainable framework that supports long-term compliance and operational performance.
Frequently Asked Questions
What is the main difference between DCS and PLC in a hospital setting?
A DCS manages continuous, multi-loop process control across large areas — such as campus-wide HVAC and energy systems — with built-in coordination between subsystems. A PLC handles discrete, logic-based sequences at the equipment level, such as generator transfer switching and sterilizer cycle control, with high-speed deterministic response. Hospitals typically use both, with DCS serving as the supervisory process layer and PLCs managing individual equipment safety logic.
Can a PLC replace a DCS in hospital HVAC control?
PLCs can manage individual HVAC equipment, but replacing a DCS for campus-wide hospital HVAC would require engineering a large network of PLCs with a separate SCADA layer to achieve comparable coordination and visibility. For facilities with hundreds of HVAC zones, this approach typically results in higher long-term engineering costs and reduced operational flexibility compared to a purpose-built DCS architecture.
Which system is better for hospital emergency power control?
PLCs are the standard choice for hospital emergency power control, specifically for Automatic Transfer Switch sequencing and generator control panels. The deterministic sub-10ms response capability of a PLC meets NFPA 99 requirements for essential electrical system transfer times, whereas DCS response latency would be insufficient for these time-critical switching operations.
How do DCS and PLC systems integrate with hospital CMMS platforms?
Both DCS and PLC systems can be integrated with CMMS platforms through OPC-UA, BACnet, or Modbus TCP protocols. This integration allows the CMMS to receive runtime hours and alarm data directly from control systems, automatically triggering preventive maintenance work orders based on actual equipment usage rather than fixed calendar schedules. CMMS platforms like Oxmaint support custom asset profiles that capture the unique maintenance requirements of DCS controllers and PLC panels.
What maintenance documentation do Joint Commission surveyors require for hospital control systems?
Surveyors require timestamped functional test records for life safety systems controlled by PLCs, including emergency generators, ATS panels, and fire suppression interfaces. For DCS-managed systems, calibration records for environmental monitoring instruments, software change logs, and alarm management documentation are typically reviewed. All records must identify the technician, test parameters, results, and any corrective actions taken.
Is a hybrid DCS and PLC architecture cost-effective for hospitals?
Yes. Hybrid architectures represent the most common approach in modern hospital automation design because they deploy each technology where its strengths are most needed. The DCS handles supervisory coordination and energy management while PLCs manage equipment-level safety logic. This approach avoids forcing either system into applications outside its natural performance envelope, resulting in better reliability and lower long-term maintenance costs than a single-technology strategy.