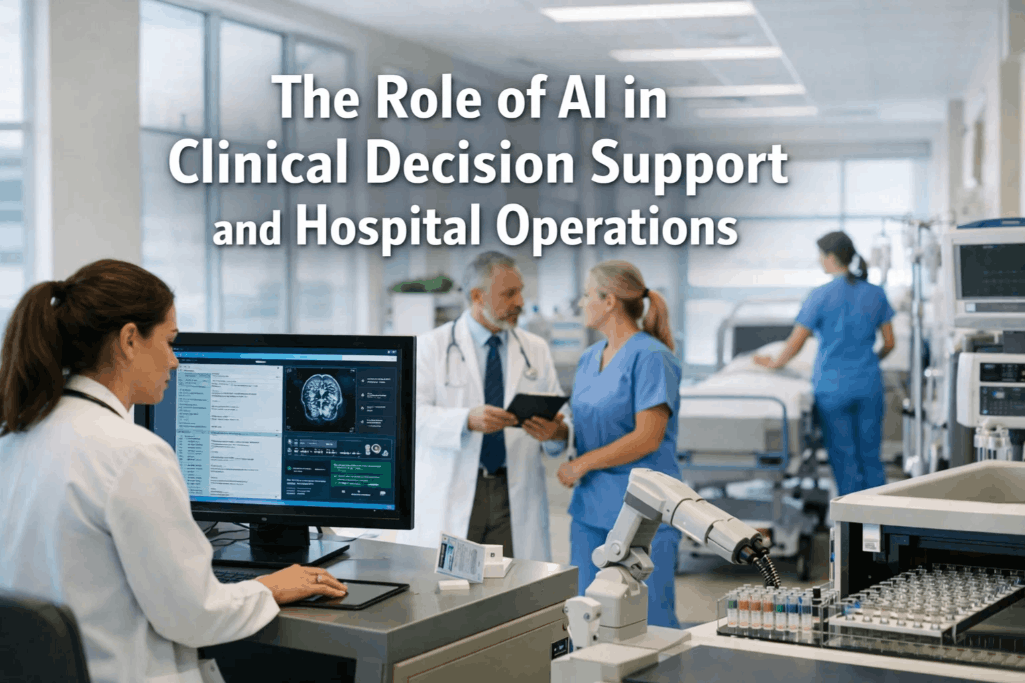
Artificial intelligence is no longer a distant promise in healthcare — it is actively reshaping how clinicians make decisions and how hospitals function at every operational level. From flagging sepsis risk hours before symptoms escalate to automatically reallocating surgical suites based on real-time throughput data, AI-driven clinical decision support and hospital operations platforms are delivering a measurable shift in both patient outcomes and institutional efficiency. The convergence of large language models, predictive analytics, and integrated workflow automation is giving hospitals tools that were simply unavailable even five years ago. For healthcare leaders evaluating where to invest next, understanding how AI applies across clinical and operational domains is no longer optional — it is foundational. Ready to see how AI-powered operations can work in your facility? start a free trial or book a demo to explore the possibilities.
Bring AI Intelligence to Your Clinical and Operational Workflows
OxMaint connects predictive analytics, asset intelligence, and automated workflows in a single platform built for the demands of modern hospital operations.
What Is AI-Powered Clinical Decision Support?
Clinical decision support systems (CDSS) have existed in some form for decades — rule-based alerts, drug interaction checkers, dosage calculators. What distinguishes modern AI-powered CDSS from these earlier tools is the ability to learn continuously from vast, heterogeneous data sources and generate probabilistic recommendations rather than static rules. Traditional CDSS asks: "Does this order violate a predefined protocol?" AI-powered CDSS asks: "Given this patient's full longitudinal record, current vitals, lab trends, and population-level outcomes data, what is the most likely trajectory, and what intervention produces the best risk-adjusted outcome?"
That distinction has profound implications for clinical practice. AI systems can surface patterns that no individual clinician — regardless of experience — could reliably detect across a full patient population. They can aggregate signals across structured EHR data, unstructured clinical notes, imaging findings, and real-time physiological monitoring simultaneously. And they can do it at the point of care, embedded in the workflows where decisions are actually made.
Core Clinical Applications of AI Decision Support
AI clinical decision support is not a single technology but a family of capabilities that addresses different phases of the patient care continuum. The applications with the strongest evidence base and the most immediate clinical impact span diagnostics, risk stratification, treatment planning, and patient monitoring.
AI-Assisted Diagnostics
Deep learning models trained on millions of labeled images now match or exceed radiologist performance on specific diagnostic tasks — detecting early-stage lung nodules, classifying diabetic retinopathy, identifying acute intracranial hemorrhage on CT scans. These models do not replace radiologists; they act as a second reader that flags high-priority findings for immediate review, reducing the time between image acquisition and diagnosis in time-sensitive conditions like stroke and pulmonary embolism.
Early Warning and Deterioration Prediction
Sepsis, acute kidney injury, and respiratory failure all have identifiable physiological precursors that appear in patient data hours before overt clinical deterioration. AI early warning systems continuously monitor vital signs, laboratory values, and nursing assessment data to generate real-time risk scores. Hospitals deploying these systems have demonstrated reductions in sepsis mortality and ICU transfer rates by enabling earlier, more targeted intervention before a patient reaches crisis.
Clinical Documentation and NLP
Natural language processing extracts structured clinical intelligence from unstructured physician notes, discharge summaries, and operative reports. AI documentation tools reduce the administrative burden on clinicians by generating draft notes from ambient recordings, pre-populating structured fields from free text, and flagging documentation gaps that affect coding accuracy and quality measure reporting. Reducing documentation burden is consistently cited as a top driver of clinician satisfaction in AI adoption surveys.
Medication Safety and Optimization
AI pharmacy intelligence goes beyond static drug interaction checking to model pharmacokinetic profiles at the individual patient level, accounting for renal function, genetic polymorphisms, concurrent medications, and body composition. These systems reduce adverse drug events by recommending patient-specific dosing adjustments and flagging combinations that carry elevated risk for a particular patient's profile — even when no standard interaction alert would be triggered.
Predictive Readmission and Discharge Planning
Machine learning models trained on historical patient journeys identify patients at elevated risk for 30-day readmission while they are still admitted, enabling proactive discharge planning, social work referrals, and post-discharge follow-up scheduling before the patient leaves the building. Reducing preventable readmissions is both a patient safety priority and a direct financial concern under value-based care payment models.
Precision Treatment Recommendations
In oncology, AI platforms now synthesize tumor genomics, molecular pathology, and population-level treatment response data to generate treatment recommendations aligned with evolving clinical guidelines. These systems ensure that every patient's case is reviewed against the full body of evidence — reducing variation in care delivery and accelerating the translation of research findings into clinical practice at the point of care.
AI in Hospital Operations: Beyond the Bedside
The operational complexity of a modern hospital — managing thousands of beds, dozens of clinical departments, hundreds of equipment assets, and thousands of staff members across overlapping care workflows — creates an environment where AI-driven optimization delivers compounding returns. Operational AI does not improve individual clinical decisions; it improves the system through which care is delivered.
AI demand forecasting models predict inpatient census, ED visit volume, and surgical case load days in advance using historical patterns, seasonal trends, community health data, and scheduled procedure pipelines. Hospitals use these forecasts to proactively adjust staffing levels, activate overflow protocols, and manage elective case scheduling to prevent boarding and diversion — problems that traditionally required reactive escalation by senior leadership.
Operating room utilization is one of the largest sources of revenue and one of the most complex scheduling challenges in hospital management. AI scheduling platforms optimize case sequencing by modeling procedure duration variability, surgeon preference patterns, sterilization turnaround times, and downstream ICU capacity to minimize gaps, reduce overtime, and increase overall room utilization without increasing staff burden or patient safety risk.
AI-powered supply chain platforms continuously model consumption patterns, vendor lead times, and clinical demand signals to maintain optimal inventory levels across a hospital's formulary and supply catalog. By replacing periodic manual counts with continuous predictive replenishment, these systems reduce both stockout events and the carrying costs associated with excess inventory — two problems that have historically coexisted in the same hospital.
AI-driven predictive maintenance integrates IoT sensor data from imaging systems, HVAC infrastructure, sterilization equipment, and patient monitoring hardware to generate failure probability scores before breakdowns occur. Rather than waiting for a ventilator or MRI to fail mid-procedure, facilities using predictive maintenance platforms can schedule interventions during planned downtime windows — reducing emergency repair costs, which run 4.8 times higher than planned maintenance, and protecting clinical revenue from unplanned equipment outages.
Nurse staffing represents the single largest operational cost line in most hospitals and is directly linked to patient safety outcomes. AI workforce platforms forecast unit-level staffing needs by shift based on predicted census, patient acuity distributions, and care hour benchmarks — enabling proactive scheduling adjustments that reduce both agency labor spending and the adverse patient outcomes associated with understaffing.
AI coding assistance and prior authorization prediction reduce the administrative friction that contributes to claim denials and delayed reimbursement. Machine learning models trained on payer behavior patterns identify high-risk claims before submission, enabling pre-submission review that reduces denial rates and accelerates cash flow — particularly important for health systems operating under thin margins in competitive markets.
Clinical Decision Support vs. Operational AI: A Comparative Overview
| Dimension | Clinical Decision Support AI | Hospital Operations AI |
|---|---|---|
| Primary User | Physicians, nurses, pharmacists | Administrators, operations managers, biomed teams |
| Core Data Sources | EHR, imaging, labs, physiological monitors | Scheduling systems, IoT sensors, supply databases, HR systems |
| Output Type | Risk scores, diagnoses, treatment recommendations | Forecasts, work orders, resource allocation recommendations |
| Patient Impact | Direct — affects individual patient care decisions | Indirect — improves system capacity and reliability |
| Regulatory Complexity | High — FDA oversight for clinical-grade AI | Moderate — primarily internal operations tools |
| ROI Horizon | 12–36 months depending on clinical workflow integration | 6–24 months through measurable cost and efficiency gains |
Key Performance Metrics for AI Healthcare Programs
Implementation Considerations for Healthcare AI Programs
Deploying AI effectively in a healthcare environment requires more than acquiring technology. Successful programs share common structural characteristics that determine whether AI capabilities translate into sustainable clinical and operational value — or become expensive experiments that fail to survive integration with real-world workflows.
Data Infrastructure and Interoperability
AI models are only as good as the data they consume. Healthcare organizations must establish clean, normalized, and accessible data pipelines from EHRs, imaging systems, lab platforms, and operational databases before meaningful AI deployment is possible. FHIR-based interoperability standards have accelerated this foundational work, but organizations still face significant integration effort when legacy systems and data silos are involved.
Clinical Workflow Integration
AI recommendations generate value only if clinicians act on them. Systems that require users to leave their primary workflow to access AI insights face adoption barriers that undermine the entire investment. Successful programs embed AI outputs directly into EHR interfaces, nursing workstations, and mobile devices — delivering actionable guidance at the precise moment a decision must be made, not as a separate consultation step.
Governance, Oversight, and Bias Mitigation
AI clinical decision tools must be governed with the same rigor as any clinical protocol. This means establishing model performance monitoring, demographic bias audits, and clinical review processes for algorithm updates. Hospitals deploying FDA-regulated AI as a medical device must additionally maintain quality management documentation that satisfies 21 CFR Part 11 and applicable software as a medical device (SaMD) requirements under the FDA's evolving AI/ML framework.
Clinician Training and Change Management
Physician trust in AI recommendations is built through transparency, not authority. Training programs that explain how models generate recommendations — and that demonstrate the evidence base behind them — outperform those that present AI as a black-box oracle. Creating feedback channels where clinicians report inaccurate recommendations improves model performance over time and builds the institutional trust necessary for sustained adoption.
Regulatory and Ethical Landscape for Healthcare AI
Healthcare AI operates within a regulatory environment that is evolving rapidly, as agencies work to establish frameworks appropriate to the unique risk profile of software that influences clinical decisions. Understanding the current landscape is essential for procurement, compliance, and risk management teams evaluating AI platforms.
The FDA's evolving framework for AI/ML-based SaMD distinguishes between locked algorithms and adaptive algorithms that update post-deployment. Clinical AI tools that influence diagnosis or treatment decisions for specific conditions fall within this framework and require either 510(k) clearance or De Novo authorization, with associated post-market surveillance obligations that continue throughout the product's lifecycle.
The ONC's 21st Century Cures Act provisions establish interoperability requirements that directly affect AI data pipeline architecture. Healthcare organizations and their AI vendors must ensure that data exchange practices supporting model training and inference comply with information blocking rules, USCDI standards, and FHIR API requirements — particularly when data flows cross organizational boundaries.
AI models trained on historically unrepresentative datasets risk perpetuating or amplifying disparities in clinical care. Regulatory attention to algorithmic bias in healthcare AI is increasing, with several states pursuing legislation that requires bias auditing for high-risk clinical AI systems. Proactive demographic performance analysis across race, ethnicity, gender, age, and socioeconomic proxies is both an ethical imperative and an emerging compliance requirement.
AI model training that uses protected health information requires a compliant legal basis under HIPAA — typically a data use agreement, de-identification per Safe Harbor or Expert Determination standards, or an IRB-approved research authorization. Operational AI tools that process PHI in real time must maintain Business Associate Agreements and implement the technical safeguards required by the HIPAA Security Rule for all data in transit and at rest.
The Integrated Vision: AI Across Clinical and Operational Domains
The most significant long-term value of healthcare AI emerges not from isolated point solutions but from integrated platforms that connect clinical intelligence with operational execution. A hospital that predicts patient deterioration but cannot rapidly mobilize the right resources to respond has captured only a fraction of the potential benefit. A hospital that optimizes surgical scheduling but cannot monitor the equipment reliability of its operating rooms is managing risk with incomplete information.
The direction of the industry is toward platforms that unify these domains — where predictive patient monitoring, equipment health tracking, capacity forecasting, and workflow automation share a common data infrastructure and a common operational interface. For hospital leaders, the strategic imperative is to evaluate AI investments not only for their individual ROI but for their ability to integrate with adjacent systems and compound their value over time. The facilities that will lead on outcomes and efficiency in the next decade are the ones making those integrated bets now. Start a free trial with OxMaint to explore how operational AI can serve as one integrated layer in your facility's broader intelligence platform, or book a personalized demo with our team today.
OxMaint: The Operational AI Layer Your Hospital Needs
Connect IoT asset intelligence, automated maintenance workflows, and audit-ready documentation in one platform — and give your operations team the same predictive power your clinical teams are building on the bedside.
Frequently Asked Questions
How does AI clinical decision support differ from traditional rule-based alerts?
Traditional rule-based CDSS fires alerts when a specific threshold is crossed — a drug interaction flag or a critical lab value. AI-powered CDSS learns probabilistic patterns from thousands of patient outcomes and generates risk scores that reflect the combined weight of many variables simultaneously. This allows AI systems to identify patients at risk before any single threshold is reached, reduces alert fatigue by generating fewer but more clinically relevant alerts, and adapts to new data as patient populations and treatment patterns evolve — something static rules cannot do.
What types of hospital operations benefit most from AI automation?
The highest-impact operational applications are those involving complex demand forecasting and resource scheduling — OR utilization, inpatient capacity management, and nursing staffing — as well as asset-intensive domains where unplanned failures carry high financial and clinical consequences, such as biomedical equipment maintenance and medical gas infrastructure. Supply chain optimization also delivers significant ROI, particularly for high-cost consumables and medications with narrow usage windows. Organizations typically start with one or two high-value use cases, demonstrate ROI, and then expand across the operational portfolio.
Is AI clinical decision support safe for direct patient care use?
Clinical AI tools that directly influence patient care decisions are subject to FDA regulatory oversight as Software as a Medical Device (SaMD), which requires clinical validation, post-market surveillance, and quality system documentation. Hospitals evaluating AI CDSS tools should verify the regulatory status of any product, review published validation studies in populations representative of their own patient mix, and establish internal governance protocols that define how clinicians should weigh AI recommendations against their own clinical judgment. AI is most safely deployed as decision support — informing, not replacing, clinician judgment.
How long does it take to implement an AI-powered hospital operations platform?
Implementation timelines vary by scope and existing data infrastructure. A focused deployment on a single operational domain — such as predictive equipment maintenance or surgical scheduling optimization — can deliver initial results within 60 to 90 days. Full-scale enterprise deployments spanning clinical, operational, and supply chain domains typically require 6 to 18 months, with the longest phases driven by EHR integration complexity and change management rather than the AI configuration itself. Cloud-based platforms have significantly reduced infrastructure setup time compared to on-premise deployments from prior generations.