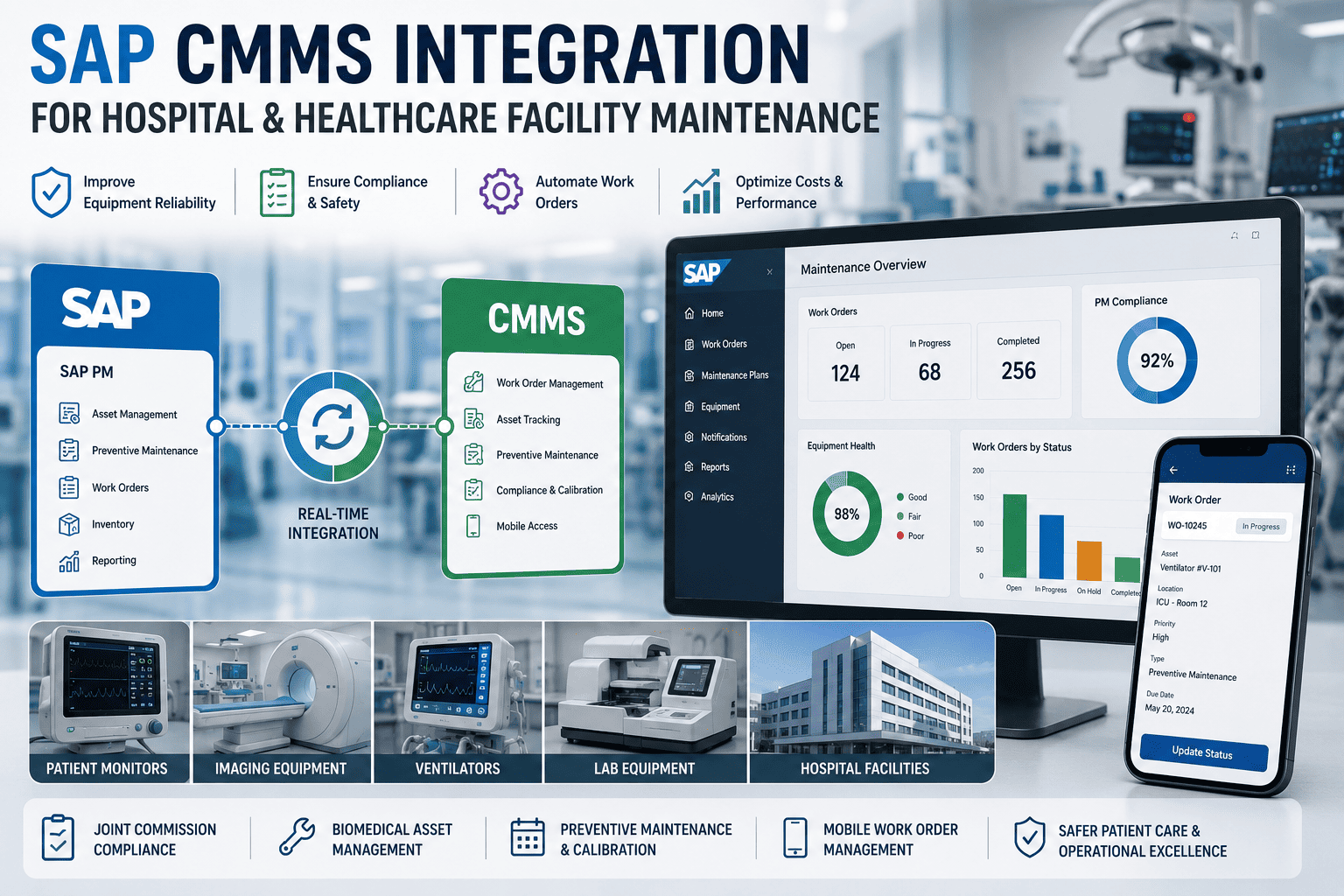
SAP CMMS Integration for Hospital and Healthcare Facility Maintenance
Hospital maintenance has different stakes from any other industry. A ventilator failure threatens a patient's life. A missed calibration triggers a Joint Commission citation. SAP PM alone was not designed for this complexity. Book a free demo to see hospital-grade integration in action.
HEALTHCARE GUIDE
SAP CMMS Integration for Hospital and Healthcare Facility Maintenance
Five risk tiers, six regulatory bodies, thousands of medical devices. The integration architecture built for the only industry where maintenance failures threaten patient lives.
5Risk tiers
6+Reg bodies
24/7Patient care
Why Healthcare Maintenance Is Different
A hospital is the only environment where maintenance directly affects whether patients live or die. Five distinct stakeholders all depend on the maintenance team performing—and each of them has a different definition of what "performing" means. Without integrated SAP-CMMS architecture, the maintenance team ends up trying to serve all five with spreadsheets, paper logs, and reactive fixes. The result is the same in every hospital that tries it: missed calibrations, compliance citations, and overworked biomedical engineers.
The 5 Stakeholders Depending on Maintenance
Each demands something different; all converge on integrated data
BIOMEDICAL ENGINEER
Demands
Real-time calibration tracking, certificate management, and instant access to device history for every IV pump, ventilator, and infusion device under their authority.
COMPLIANCE OFFICER
Demands
Audit-ready records with full traceability for every device. Joint Commission, FDA, CMS, and state inspections must move from week-long crises to one-day reviews.
FACILITIES DIRECTOR
Demands
Lifecycle cost visibility against capital and operating budgets. Asset replacement planning that aligns with regulatory cycles and budget approval timelines.
CLINICAL STAFF
Demands
Equipment available the moment patients need it. Devices that have just been serviced should not be the ones with errors. Predictable, communicated maintenance windows.
CIO / IT LEADERSHIP
Demands
Integrated data flow without manual reconciliation between SAP, CMMS, and EHR systems. Single source of truth for asset performance reporting to leadership.
No single system serves all five demands in isolation. Integration is the only architecture that does.
The five-stakeholder pressure is unique to healthcare. No other industry combines life-safety stakes, regulatory burden, multi-departmental complexity, and 24/7 operations the way a hospital does. Maintenance teams ready to assess their stakeholder coverage can sign up free to run the healthcare maintenance diagnostic against their current operations.
The Medical Equipment Risk Tier System
Not every hospital device deserves the same maintenance attention. A defibrillator failure threatens a life; a wheelchair wheel needs grease but won't kill anyone. The integration architecture works because it categorizes equipment into five risk tiers, each with its own PM frequency, regulatory framework, and integration priority. The pyramid below shows the model—highest risk at the top, broadest base at the bottom.
Medical Equipment Risk Tier Pyramid
Five tiers · risk decreases as device count increases
1
LIFE
Life-Critical
VentilatorsDefibrillatorsAnesthesiaECMO
PM monthly · FDA Class III · AAMI
2
HIGH
Diagnostic Critical
MRICT scannersUltrasoundMammography
PM quarterly · FDA Class II · ACR accreditation
3
MED
Therapeutic Support
Infusion pumpsPatient monitorsDialysisTelemetry
PM semi-annual · FDA Class II
4
LOW
General Clinical
Hospital bedsScalesWorkstationsBasic monitors
PM annual · general medical device regulations
5
SYS
Facility Systems
HVACGeneratorsWater systemsElectrical
PM quarterly · ASHE · OSHA · EPA
Tier 1 carries 5% of device count but 80% of patient-safety risk. Integration priority follows that math—Tier 1 deploys first, Tier 5 last.
The risk tier model matters because it determines integration sequencing. A hospital that tries to deploy CMMS coverage across all 2,000+ devices simultaneously typically stalls. A hospital that deploys Tier 1 first, then progressively expands, delivers measurable patient-safety improvements within months. Hospitals ready to map their device inventory against the five-tier framework can sign up free to run a tier-based readiness audit.
Joint Commission Compliance Through Integration
The Joint Commission's Environment of Care chapter (EC) defines the maintenance standards every accredited US hospital must meet. The standards are not abstract; they map directly to specific integration capabilities. The coverage stack below shows which JC standards each integration capability satisfies—giving compliance officers a direct line from system design to audit readiness.
EC.02.04.01
Equipment Management Plan
Integration delivers
Documented inventory of all medical equipment with criticality classification, maintenance strategy, and ownership clearly assigned.
EC.02.04.03
Inspection & Testing Records
Integration delivers
Time-stamped work order records with technician identity, parts used, test results, and pass/fail status for every device intervention.
EC.02.05.05
Utility Systems Maintenance
Integration delivers
Tier 5 facility system coverage with redundancy validation, generator testing schedules, and water system documentation per ASHE guidelines.
AEM Program
Alternate Equipment Maintenance
Integration delivers
Risk-based maintenance intervals supported by device-level failure history. Deviation from manufacturer schedules requires data justification—integration provides it.
FDA Recalls
Device Recall Management
Integration delivers
UDI-tagged device tracking enables instant identification of recalled units and documented remediation actions for each affected asset.
Compliance officers running their next Joint Commission survey simulation can use this framework to identify which integration gaps will surface as findings. Hospitals approaching a survey window can book a free demo for a compliance-readiness walkthrough against the five standards above.
Run the Healthcare Maintenance Assessment
A 30-minute working session walks through your device inventory, risk tier distribution, and Joint Commission compliance posture—producing a prioritized integration plan that addresses your hospital's specific gap profile.
Hospital integration differs from manufacturing in three critical ways: the rollout cannot disrupt active patient care, biomedical engineering owns the device side while facilities owns the building side (and they need to coordinate), and every phase must produce compliance documentation. The roadmap below is tuned for these realities.
P1
Week 1–3
Device Inventory & Risk Tier Assignment
Complete inventory across all clinical departments. Assign each device to one of the five risk tiers. Verify SAP master data for top-tier devices. Document compliance scope—which devices fall under which regulatory frameworks.
Bring biomedical engineering, facilities, compliance, IT, and clinical leadership into design sessions. Map workflows for each stakeholder. Resolve ownership questions—who closes work orders, who approves PM deviations, who responds to alerts.
Output: stakeholder-approved workflow diagrams
P3
Week 7–10
SAP-CMMS Integration Build & UDI Mapping
Configure the connector between SAP PM and the CMMS execution layer. Map UDI codes to functional locations. Build calibration certificate tracking workflows. Test edge cases including recall workflows and AEM exception handling.
Output: working integration with verified compliance pathways
P4
Week 11–13
Tier 1 Pilot in Critical Care Departments
Activate integration on Tier 1 devices in ICU, OR, and emergency department first. Train biomedical engineers on mobile workflows. Monitor without disrupting clinical operations. Refine before expanding.
Output: validated workflow with measurable compliance lift
P5
Week 14–18
Tier-by-Tier Hospital-Wide Rollout
Expand to Tiers 2 through 5 in priority order. Onboard remaining biomedical and facilities staff. Activate analytics and audit-readiness reporting. Begin the continuous improvement cycle aligned with Joint Commission survey windows.
Output: hospital-wide architecture at 95%+ compliance
The 18-week timeline assumes reasonable SAP master data quality and an engaged biomedical engineering team. Hospitals starting from paper-based maintenance records typically add 4–6 weeks for inventory digitization at the front of the project. Healthcare leaders ready to walk through this plan against their facility specifics can sign up free to model the 18-week rollout for their hospital.
Hospital-Grade Maintenance Integration
Oxmaint integrates with SAP PM, supports the five risk tiers, and delivers Joint Commission audit-readiness as a native capability—not a custom add-on. Built for healthcare's stakeholder complexity from the architecture up.
How does SAP-CMMS integration help with Joint Commission compliance?
The integration maps directly to the JC Environment of Care standards. EC.02.04.01 requires a documented equipment management plan—integration provides a tiered device inventory with maintenance strategy per device. EC.02.04.03 requires inspection and testing records—integration delivers timestamped work orders with technician identity and test results. AEM programs require risk-based maintenance justification—integration supplies the device-level failure history needed. Most accredited hospitals find that integration reduces survey preparation time from weeks to a few days.
Which medical devices should we prioritize for integration first?
Tier 1 life-critical devices—ventilators, defibrillators, anesthesia machines, infusion pumps in ICU settings—deliver the fastest patient-safety improvement. These devices typically represent 5–10% of total device count but 70–80% of regulatory and patient-safety exposure. Tier 2 imaging equipment comes next because of its compliance footprint (ACR accreditation, radiation safety). Tier 5 facility systems should integrate alongside Tier 1 because of life-safety code requirements around backup power and water quality.
How is healthcare CMMS different from manufacturing CMMS?
Three things change at the same time. First, devices are mobile—a ventilator moves between ICU, OR, and recovery, so location tracking matters more than fixed-asset thinking. Second, calibration documentation is regulatory, not optional—every action needs the technician's identity, the test result, and a chain-of-custody record. Third, the integration must coexist with active patient care—maintenance windows are tighter, scheduling is harder, and the consequence of disruption is direct patient harm. The architecture is similar to manufacturing integration, but the workflow and documentation requirements are categorically different.
Can we integrate without disrupting active patient care?
Yes, when the rollout is sequenced correctly. The integration runs in parallel with existing systems during the pilot phase, so clinical workflows continue uninterrupted. Cutover to the integrated platform happens device-by-device during scheduled PM windows, not during patient use. Tier-by-tier deployment further protects clinical operations—Tier 1 devices in critical care departments deploy first under tightest controls, with lower-tier devices following once the workflow is proven. Most hospitals complete the full transition without a single clinical disruption.
What's the typical ROI for hospital integration projects?
For a mid-sized hospital with 2,000–3,000 devices, first-year implementation typically runs $500K–$1.2M depending on scope and SAP environment complexity. Annual benefits run $2M–$4M, driven primarily by compliance cost reduction (audit prep, citation avoidance), biomedical engineering productivity gains (40–60% less administrative time), and avoided device-failure incidents. Payback periods cluster around 9–15 months. The largest benefits often come from compliance posture improvements that are hard to quantify upfront but prevent expensive findings during survey.